Tue, 23 August 2016
We cover several excellent post on rashes, including:
Next, we dive into core content on platelet problems including problems caused by drugs, immune thrombocytopenic purpura (ITP/idiopathic thrombocytopenic purpura) and thrombotic thrombocytopenic purpura (TTP) using Tintinalli Chapter 233 (8th ed) and Rosen's Chapter 122 (7th ed) as a guide.
Thanks for listening! Jeremy Faust and Lauren Westafer |
Mon, 8 August 2016
We cover ultrasound guided pericardiocentesis using the posts from EMin5, CoreEM, and the Ultrasound Podcast. Then, we delve into core content on the pericardium using Rosen’s (8th ed) Chapter 82 and Tintinalli (8th ed) Chapter 55 covering pericardial effusions, pericarditis, and myocarditis.
Thanks for listening! Jeremy Faust & Lauren Westafer |
Sun, 17 July 2016
We cover a post by Dr. Rory Spiegel, EMNerd: The Case of Differing Perspectives, on the results of the ATACH-2 trial on blood pressure control in intracranial hemorrhage (ICH). This study sought to determine the safety and efficacy of the Population: adults (>18 y/o) with ICH on CT scan, GCS ≥ 5 and <4.5 hours since symptom onset (changed mid-study) Intervention: Reduce and maintain the hourly minimum systolic blood pressure in the range of 110 to 139 mm Hg throughout the period of 24 hours after randomization ("intensive treatment"). Preferred agents for blood pressure control in order of preference were 1. nicardipine 2. labetalol (diltiazem or urapidil if not available)
Control: Reduce and maintain the hourly minimum systolic blood pressure in the range of 140 to 179 mm Hg throughout the period of 24 hours after randomization.
Outcome: The primary outcome was the proportion of patients who had moderately severe or severe disability (modified Rankin scale score (mRS) 4-5) or those who had died (mRS 6; hereafter referred to as “death or disability”) at 3 months.
We also discuss the history of blood pressure control in ICH and the pendulum swing on this in recent years, using an episode of the Skeptic's Guide to Emergency Medicine, Episode 73. This episode covers the Interact-2 trial. Core Content We delve into core content on ICH using Rosen’s (8th ed) Chapter and Chapter in Tintinalli (8th ed). We also discuss the PATCH trial with regard to ICH management in patients on antiplatelet agents, discussing a REBELEM post on this trial.
|
Fri, 1 July 2016
Just in time for the new interns, we answer the most common question asked of us - our favorite resources to use on shift. Free Open Access Medical Education (FOAM) exists in forms that are suitable for self-study or function as resources and those that are easy to use resources to consult on shift, Just In Time (JIT) Resources. We review our favorite FOAM JIT resources.
Direct download: FOAMcastini_July_1_Just_in_time_FOAM.mp3
Category:general -- posted at: 11:35am EDT |
Sun, 26 June 2016
We cover a Scancrit post on the Back Up Head Elevated (BUHE) intubation position. This post details a multicenter retrospective observational study by Khandelwal et al in Anesthesia & Analgesia. Intubating with the head elevated (ear to sternal notch) and the back of the bed up reduces complications. We delve into core content on the esophagus using Rosen’s (8th ed) Chapter 71 and Chapter 77 in Tintinalli (8th ed). We discuss dysphagia, food impaction, and esophagitis.
JEremy Faust and Lauren WEstafer
Direct download: Foamcast_52_Back_up_head_elevated_intubation_-_6-25-16_5.17_PM.mp3
Category:general -- posted at: 8:56am EDT |
Thu, 16 June 2016
We cover pearls from smaccDUB (Social Media and Critical Care Conference in Dublin, Ireland), Day 3. We are here thanks to the Rosh Review. Dr. Scott Weingart - "Post-Intubation Sedation"
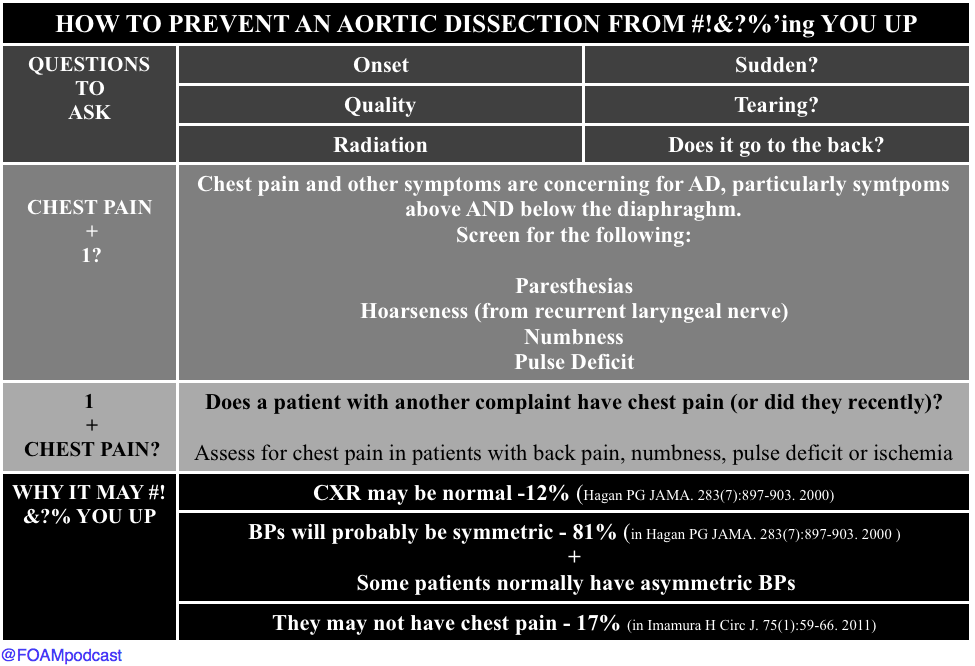
Dr. David Carr - "The Aorta Will #!&?% You Up" Dr. Kathleen Thomas - "Oh Sh**! They’re bombing the hospital!" We should not need a website entitled STOPBOMBINGHOSPITALS.ORG but, unfortunately, over the past 4 years, 400 hospitals have been bombed. This passionate, wrenching talk is a "must see" and "must listen" when the free talks are released on the SMACC podcast over the course of the next year. ive use in the emergency department. Emergency medicine journal : EMJ. 30(11):893-5. 2013. [pubmed]
Direct download: Foamcastini_smaccdub_day_3_aorta_and_pain.mp3
Category:general -- posted at: 2:01pm EDT |
Wed, 15 June 2016
#smaccDUB day 2 Dr. Reuben Strayer - “Disruption, Danger, and Droperidol: Emergency Management of the Agitated Patient." Dr. Strayer presented a brilliant talk on dealing with the quintessential Emergency Medicine patient - the undifferentiated acutely agitated patient. These patients are high risk and require emergent stabilization and resuscitation. Dr. Haney Mallemat - "The PEA Paradox" The typical way we think about PEA, the "H's and T's," is overly complicated. Further, we are horrendous at pulse palpation (see this for more), and so what we think is PEA may not actually be PEA. Dr. Mallemat proposed QRS duration as one way to think about PEA, although this has limitations. Dr. Michele Dominico - "How Usual Resuscitative Maneuvers Can Kill Paediatric Cardiac Patients" Interventions we jump to in sick patients - oxygenation, ventilation, vasopressors - these can kill pediatric patients with cardiac pathology. She gave examples of some high yield pearls in these already terrifying patients. EM Literature update by Drs. Ashley Shreves and Ryan Radecki
Interesting and Ridiculous Research Pearls from Drs. Ashley Shreves and Ryan Radecki
|
Tue, 14 June 2016
We are at SMACC in Dublin - thanks to the Rosh Review, an excellent board review question bank. Here are some of our favorite pearls. Do We Make Saves? Dr. Mervyn Singer "Is Survival Predetermined in the Critically Ill?"
Favorite Pearls Dr. Suzanne Mason - "Acute Care of the Elderly"
Dr. Victoria Brazil - "So You Think You're a Resuscitationist?"
Direct download: FOAMcastini_SmaccDub_Saves_day_1_-_6_14_16_7.56_PM.mp3
Category:general -- posted at: 3:05pm EDT |
Thu, 9 June 2016
We cover this short video from EMRAP on lateral canthotomies. This is one of those rare procedures that is vision saving; hence, it is worthy of frequent review. Then, we delve into core content on orbital fractures, hyphemas, and ocular burns using Tintinalli and Rosen's Emergency Medicine as a guide. Show notes and references at foamcast.org Thanks for listening! Jeremy Faust and Lauren Westafer |
Tue, 24 May 2016
We review the FOAM video by Dr. Anna Pickens of EMin5.com on "Special Seizures" including hyponatremia, isoniazid toxcitiy, alcohol withdrawal, and eclampsia.
Jeremy Faust and Lauren Westafer |
FOAMcast - An Emergency Medicine Podcast

Categories
generalmedicine, urology, emergency medicine
medicine, emergency medicine, toxicology, foam, emergency medicine resident
transfusions
medicine, psychiatry, ICP, emergency medicine
emergency medicine, foam, hepatic emergencies
acid-base
electrolytes
pregnancy
infectious disease
allergy
toxicology
cardiology
neurology
trauma, spleen
conferences, FOAM, smacc
environmental, emergency medicine
medicine, cardiology, toxicology, emergency medicine
ortho
statistics
emergency medicine, neurology
respiratory
gastroenterology
Archives
FebruaryDecember
October
September
March
February
January
December
October
September
July
June
March
January
December
November
October
September
August
July
June
April
March
February
January
December
November
October
September
August
July
June
May
April
March
February
January
December
October
September
July
May
April
March
February
January
December
November
October
September
August
July
June
May
April
March
February
January
December
November
October
September
August
July
June
May
April
March
February
January
December
November
October
September
August
July
June
May
April
March
February
January
December
November
October
September
August
July
June
May
April
March
February
January
December
November
October
September
August
July
June
May
| S | M | T | W | T | F | S |
|---|---|---|---|---|---|---|
| 1 | 2 | |||||
| 3 | 4 | 5 | 6 | 7 | 8 | 9 |
| 10 | 11 | 12 | 13 | 14 | 15 | 16 |
| 17 | 18 | 19 | 20 | 21 | 22 | 23 |
| 24 | 25 | 26 | 27 | 28 | 29 | 30 |
Syndication